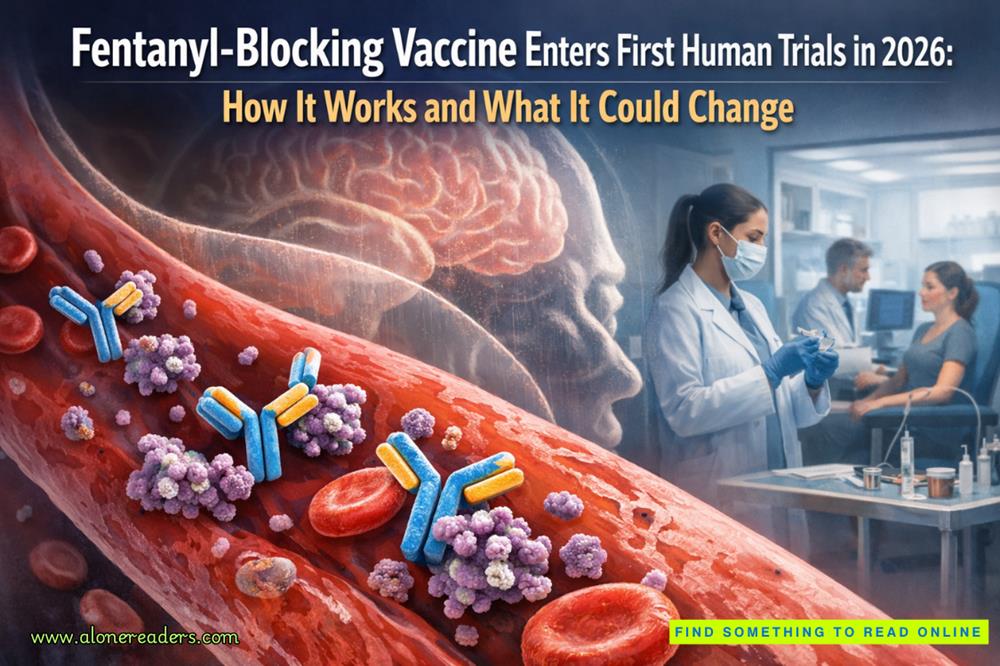
In early 2026, a milestone long discussed in addiction science and public-health policy will finally arrive: the first large, clearly defined first-in-human clinical trial of a vaccine designed specifically to block fentanyl. Unlike traditional vaccines that prevent infection, this new class of immunotherapy targets a synthetic opioid that has driven unprecedented overdose mortality across North America and beyond. The upcoming trial represents a convergence of immunology, neuroscience, military-funded biomedical research, and urgent civilian need, and it marks a shift in how medicine may confront the deadliest phase of the opioid epidemic.
The vaccine at the center of the 2026 trial was originally developed with funding from the U.S. Department of Defense, reflecting long-standing concerns about synthetic opioids not only as drugs of abuse but also as potential chemical threats. That program has since been licensed to a startup, ARMR Sciences, which plans to conduct a Phase I/II study at the Centre for Human Drug Research in the Netherlands. The choice of site is deliberate. Early-phase trials of novel neuroactive interventions demand tightly controlled environments, sophisticated pharmacology infrastructure, and extensive experience in first-in-human safety assessments. This study will enroll approximately 40 healthy adult volunteers, a typical size for a combined Phase I/II design where the primary goals are safety, tolerability, and biological proof of concept rather than clinical efficacy in real-world overdose prevention.
What distinguishes this vaccine from previous approaches to opioid addiction is its mechanism. Rather than acting on brain receptors like methadone, buprenorphine, or naltrexone, the vaccine works entirely in the bloodstream. It is built by chemically linking small fentanyl-derived fragments, known as haptens, to a carrier protein called CRM197, a deactivated form of diphtheria toxin widely used in licensed conjugate vaccines. An immune-stimulating adjuvant, dmLT, is added to amplify antibody production. Together, these components train the immune system to recognize fentanyl as a foreign molecule and to produce high-affinity antibodies that bind it rapidly after it enters the bloodstream.
The implications of this design are profound. Fentanyl’s lethality stems from its speed and potency. Because it is highly lipophilic, it crosses the blood–brain barrier within seconds, activating mu-opioid receptors in the brainstem and suppressing respiration. The vaccine-induced antibodies are intended to intercept fentanyl molecules before they can reach the central nervous system. Once bound to antibodies, fentanyl becomes too large to cross the blood–brain barrier efficiently, blunting or eliminating its psychoactive and respiratory-depressant effects. In preclinical rat studies, this strategy prevented classic opioid outcomes such as analgesia, euphoria, and fatal respiratory depression, even at doses that would normally cause overdose.
These animal results are the scientific foundation for moving into human testing, but the 2026 trial is deliberately cautious in scope. Participants will not be individuals with opioid use disorder, nor will the study attempt to measure reductions in overdose risk. Instead, researchers will focus on adverse events, immune response profiles, and the consistency of antibody generation across participants. Blood samples will be analyzed for anti-fentanyl antibody titers, binding strength, and duration of response. One of the key unknowns is how robust and durable the immune response will be in humans compared to animals, and whether booster doses will be required to maintain protective antibody levels.
Later stages of the trial may include carefully supervised administration of medical-grade fentanyl in a controlled clinical setting. Such challenge studies, if approved by ethics committees, would allow researchers to observe whether vaccinated individuals show reduced physiological and subjective responses to fentanyl compared to baseline. Measurements could include respiratory rate, oxygen saturation, pupil constriction, and subjective reports of sedation or euphoria. These data would not demonstrate real-world effectiveness, but they would provide critical evidence that the antibodies generated by the vaccine meaningfully alter fentanyl’s pharmacological effects in humans.
The ARMR-led study is not the only fentanyl-vaccine effort approaching the clinic. A separate program developed at the University of Houston, commercialized under the name “Fentanyl Armour” by Ovax, has announced plans for Phase I trials as early as 2025. That program uses a conceptually similar antibody-based approach, though with differences in hapten design and formulation. Media coverage of the Houston program has at times suggested rapid availability, but experts caution that early-phase trials are only the beginning of a long regulatory process. Even under optimistic assumptions, widespread clinical use would require successful Phase II and Phase III trials demonstrating not only biological effect but meaningful reductions in harm among people at risk.
The renewed attention to opioid vaccines reflects a broader reassessment of how societies address synthetic opioids. Traditional pharmacotherapies for opioid use disorder are effective, but they depend on adherence, access, and ongoing engagement with healthcare systems. A vaccine, by contrast, could offer long-lasting protection independent of daily medication use. This has led some researchers to envision the vaccine as an adjunct rather than a replacement for existing treatments, potentially useful for people in early recovery, individuals leaving incarceration, or patients prescribed opioids for pain who face elevated overdose risk due to fentanyl contamination.
At the same time, the concept raises complex ethical and practical questions. Vaccination against a drug of abuse challenges traditional definitions of consent, autonomy, and public-health intervention. Because the vaccine does not block all opioids equally, individuals could theoretically attempt to override its effects by taking higher doses or switching to different substances, increasing other risks. There are also concerns about whether such a vaccine could be misused in coercive contexts, such as mandated treatment or criminal justice settings. These issues are not addressed by the 2026 trial, but they loom large over any future deployment.
From a scientific standpoint, one of the most important outcomes of the 2026 study will be clarity on immune variability. Human immune responses differ widely based on genetics, age, prior exposures, and health status. A vaccine that produces strong antibody responses in some individuals but weak responses in others would face challenges in standardization and dosing. Researchers will analyze not only average antibody levels but also the distribution of responses, looking for predictors of strong or weak immunity. This information will guide future trial design and may influence whether personalized dosing strategies are needed.
Another critical question is duration. Preclinical studies suggest antibody levels decline over time, implying the need for booster shots. Determining the optimal booster schedule will be essential, particularly if the vaccine is envisioned as a tool for long-term risk reduction rather than short-term intervention. The Phase I/II design allows for extended follow-up, giving investigators early signals about how quickly antibody titers wane and whether memory immune responses are robust.
The geopolitical and institutional context of the vaccine’s development also matters. Defense funding accelerated early research, but civilian commercialization now places the program within conventional pharmaceutical pathways. Conducting the first major trial in Europe underscores the global nature of the fentanyl crisis, which increasingly affects markets beyond the United States through illicit synthetic opioid supply chains. Success in the Netherlands could pave the way for multinational trials and regulatory submissions across multiple jurisdictions.
It is important to emphasize what the 2026 trial will not show. It will not demonstrate that the vaccine prevents overdose deaths in the community. It will not address social determinants of addiction, illicit drug supply dynamics, or access to treatment. It will not be a standalone solution to the opioid epidemic. What it can do is establish whether a long-theorized biological strategy is safe and feasible in humans. If successful, it opens a new branch of addiction medicine focused on immunological interception rather than receptor modulation.
For clinicians and policymakers, the significance of this moment lies in optionality. The opioid crisis has been marked by cycles of optimism and disappointment, from painkiller reformulations to abuse-deterrent technologies. A fentanyl-blocking vaccine is not a cure, but it represents a fundamentally different angle of attack. The fact that multiple programs are converging on human trials in 2025–2026 suggests that the science has matured beyond speculation.
As early 2026 approaches, expectations should remain measured but attentive. The trial’s results will likely be incremental, reported in immunological metrics rather than dramatic clinical outcomes. Yet even incremental confirmation that humans can safely generate antibodies capable of neutralizing fentanyl would be a landmark achievement. It would validate years of preclinical work and justify the much larger, more complex trials needed to test real-world impact.
In the broader narrative of drug policy and medical innovation, the first-in-human fentanyl vaccine trial marks a turning point from reactive overdose response toward proactive biological defense. Whether this approach ultimately becomes a practical tool will depend on data still years away. For now, the scheduled start of the 2026 trial signals that an idea once confined to laboratory animals is stepping into the clinic, carrying with it both scientific promise and the weight of a public-health emergency that demands new solutions.
October 25, 2023
January 02, 2025


 Top 10 Highest-Paid Professions in the United States (2025): Salaries, Roles, and Career Paths
Top 10 Highest-Paid Professions in the United States (2025): Salaries, Roles, and Career Paths
 Top 10 Largest U.S. Companies by Revenue in 2025 (Fortune 500 Analysis)
Top 10 Largest U.S. Companies by Revenue in 2025 (Fortune 500 Analysis)
 Top 10 Highest-Earning Global Tech Companies in 2025: Revenue, Strategy, and Market Power
Top 10 Highest-Earning Global Tech Companies in 2025: Revenue, Strategy, and Market Power
 Top 10 Highest-Earning Mobile Apps in 2025: Revenue, Monetization, and Market Dominance
Top 10 Highest-Earning Mobile Apps in 2025: Revenue, Monetization, and Market Dominance
 ZombieAgent: Inside the Zero-Click AI Attack That Turns ChatGPT Agents into Persistent Data-Leaking Zombies
ZombieAgent: Inside the Zero-Click AI Attack That Turns ChatGPT Agents into Persistent Data-Leaking Zombies
 China’s Urban Air Is a Hidden Plastic Reservoir: Inside the Microplastic Clouds Over Megacities
China’s Urban Air Is a Hidden Plastic Reservoir: Inside the Microplastic Clouds Over Megacities
 The Abu Ghraib Scandal, Iraq, 2004: A Human Rights Disaster That Shook the World
The Abu Ghraib Scandal, Iraq, 2004: A Human Rights Disaster That Shook the World
 The Disbanding of the CNRP, Cambodia, 2017: Hun Sen's Clampdown on Democracy and the Reshaping of Cambodian Politics
The Disbanding of the CNRP, Cambodia, 2017: Hun Sen's Clampdown on Democracy and the Reshaping of Cambodian Politics
 The Firing of James Comey, United States, 2017: Trump's Controversial Decision Amid FBI Investigation
The Firing of James Comey, United States, 2017: Trump's Controversial Decision Amid FBI Investigation
 The Rwandan Refugee Crisis, Central Africa, 1994: Aftermath of Genocide and the Humanitarian Catastrophe
The Rwandan Refugee Crisis, Central Africa, 1994: Aftermath of Genocide and the Humanitarian Catastrophe
 The Most Important Turning Points of the Battle of Hastings (1066)
The Most Important Turning Points of the Battle of Hastings (1066)
 Why William Won the Battle of Hastings and Harold Lost: Strategy, Leadership and Fate in 1066
Why William Won the Battle of Hastings and Harold Lost: Strategy, Leadership and Fate in 1066
 How King Harold II Died: Facts, Myths, and Historical Debate
How King Harold II Died: Facts, Myths, and Historical Debate
 The Battle of Hastings: A Complete Timeline of the Fighting
The Battle of Hastings: A Complete Timeline of the Fighting
 High-End Talent Category A Work Permit China 2026: Complete Eligibility, Benefits, Application Process, and Expert Guide
High-End Talent Category A Work Permit China 2026: Complete Eligibility, Benefits, Application Process, and Expert Guide
 Cultural Activities Visa Japan 2026 Guide: Complete Eligibility, Requirements, Application Process, and Expert Tips
Cultural Activities Visa Japan 2026 Guide: Complete Eligibility, Requirements, Application Process, and Expert Tips